The why and the what
- It is about the creation of a NEW nursing process that is a little more comprehensive.
- Here are the new clinical judgment cognitive skills you are expected to have:
- Recognize Cues: What matters most to save the patient NOW? What are the priorities?
- Analyze Cues: What do the current probems/vital signs/abnormal findings mean?
- Prioritize Hypothesis: Where do I start to solve the problems/abnormal findings? What do I have to follow up immediately and what can wait?
- Generate Solutions: What can I do to make it better or to prevent complications?
- Take Action: What action/actions will I take now?
- Evaluate Outcomes: Did my nursing interventions help or has the client’s condition declined? How do I know?
- Don’t worry. We will go through each one of these cognitive skills. We will provide examples.

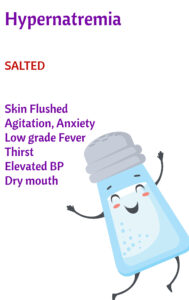
The world of mnemonics is not perfect. If the client has hypernatremia due to dehydration, the client will not be edematous.
If the client has hypernatremia due to diabetes insipidus, the client may have large amounts of urine output.
Water follows sodium. In clients with heart failure and renal failure, you want to limit sodium to prevent fluid retention.
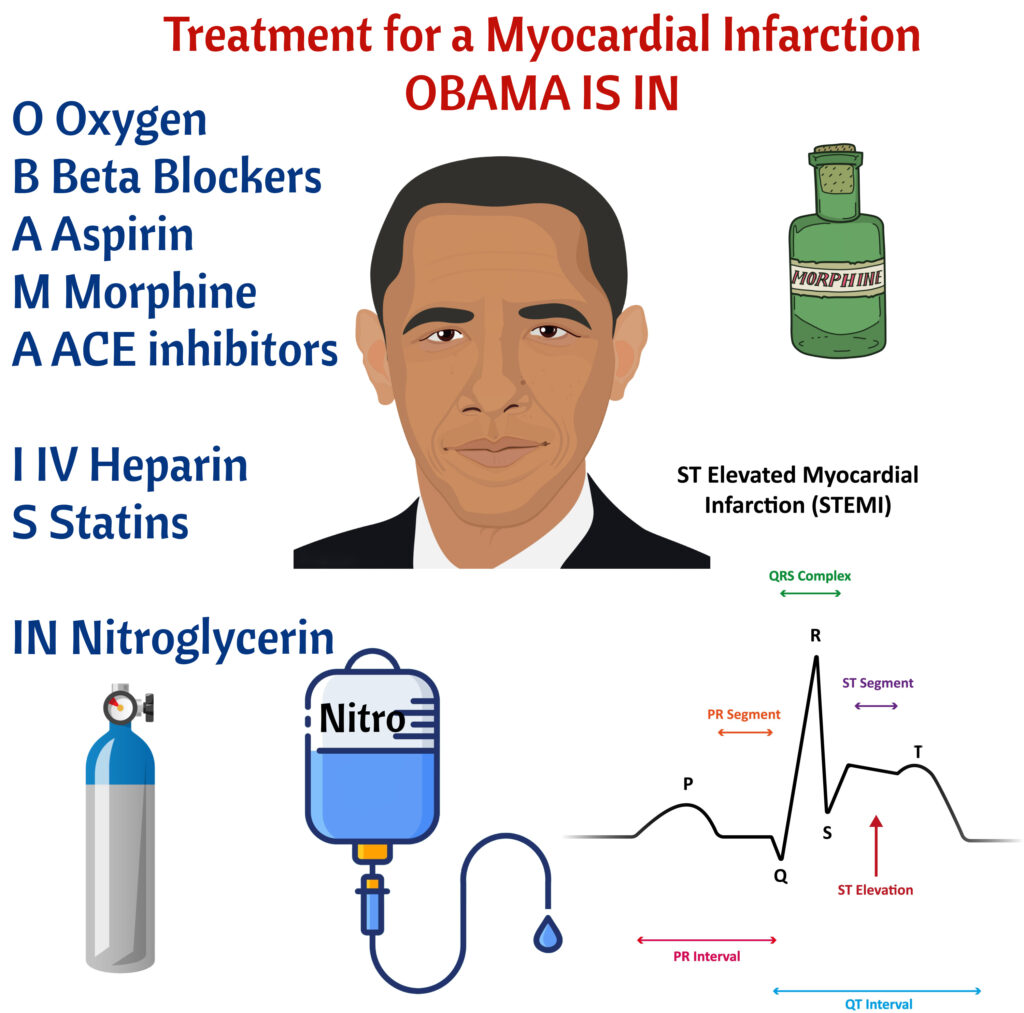
Miosis (pin point pupils)
Orthostatic Hypotension
Respiratory Depression
Physical Dependence
Hypotension/histamine release
Increased ICP!
Naloxone antidote. Remember antidote!
Euphoria and sedation

Breasts
Uterus
Bowels
Bladder
Lochia
Episiotomy/laceration/C-section
DVT
Somebody commented
“What about Homan’s sign”
so I changed it to BUBBLED. D for DVT

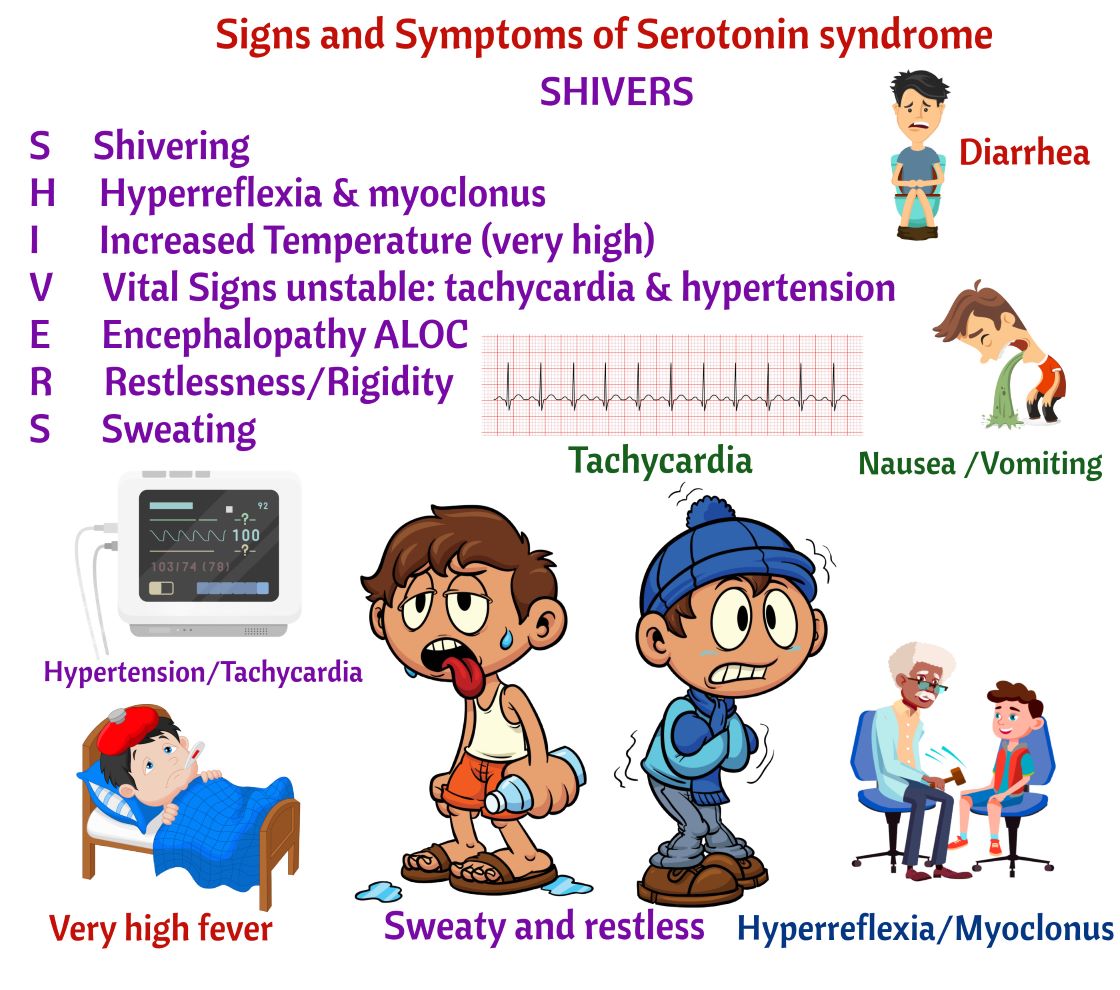
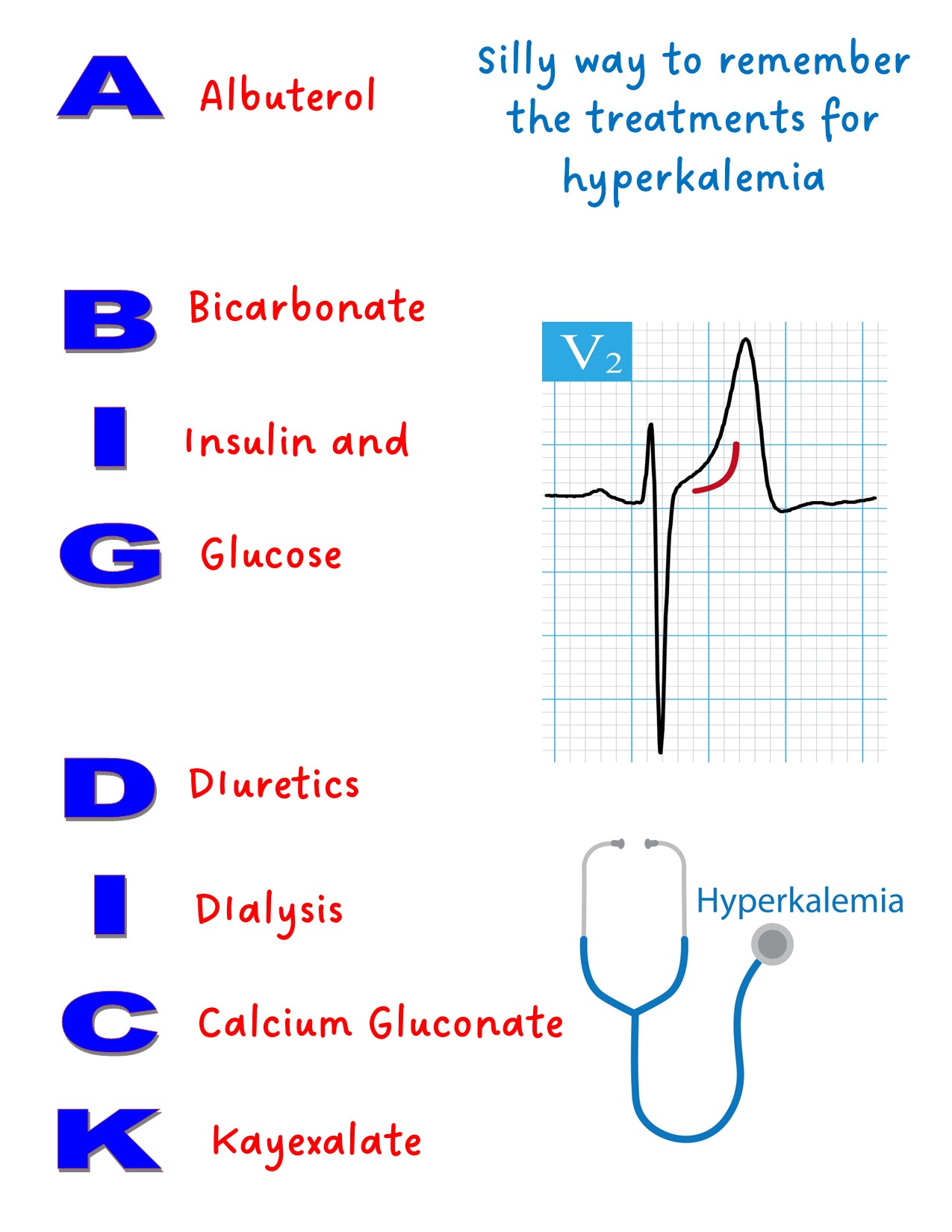
Tachycardia
Irritability
Restlessness
Excessive Hunger
Diaphoresis
Muscle weakness
Urine little or none
Respiratory depression
Decreased cardiac contractility or bradycardia
EKG changes (peaked T wave
Reflexes hyperreflexia or areflexia

Constipation Can’t shit
Urinary Retention Can’t pee
Dry Mouth Can’t spit
Dilated Pupils Can’t See