Side-lying or low semi-fowlers with legs drawn towards the chest
Monitor for Rupture
Pain that suddenly goes away without intervention
Avoid
Avoid laxatives and enemas
Avoid
Heat/Heating pad for pain management. It can lead to rupture.
Let's talk about it again!
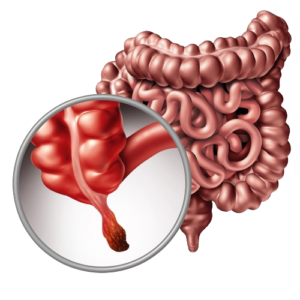
RLQ pain: Mcburney’s Pointw/ rebound tenderness.
Rovsing’s sign: RLQ elicited by palpation the the left lower quadrant.
Constant, steady pain. Pay attention: constant and steady pain. NOT comes and goes. Begins in epigastrium or periumbilical area and moves to RLQ. Steady and constant.
Low grade fever, n/v, and elevated WBCs
If ruptures: peritonitis, fever, chills, tachycardia, tachypnea, restlessness, pallor, progressive abdominal distention and guarding.
Position to relieve pain: On back with legs drawn up towards the abdomen.
Avoid applying heat because it can rupture appendix. If appendix ruptures, the client will have a penrose drain after surgery.
WARNING:If pain suddenly goes away: Appendix has RUPTURED!
NO ENEMAS, KEEP NPO, NO PO MEDS, GIVE IV FLUIDS/MEDS, NO WARM COMPRESSES, MEASURE ABDOMINAL GIRTH.
Treatment: Appendectomy
Best position for a client with an appendectomy is right side-lying or semi-fowlers.
Test your Understanding
A 12-year-old female presents with sudden onset of severe abdominal pain. The pain started in the periumbilical region and migrated to the right lower quadrant over the last 12 hours. She reports nausea, vomiting, anorexia, and has not had a bowel movement for 48 hours. Physical examination reveals rebound tenderness, guarding, and positive Rovsing’s sign. Her vital signs are within normal limits.