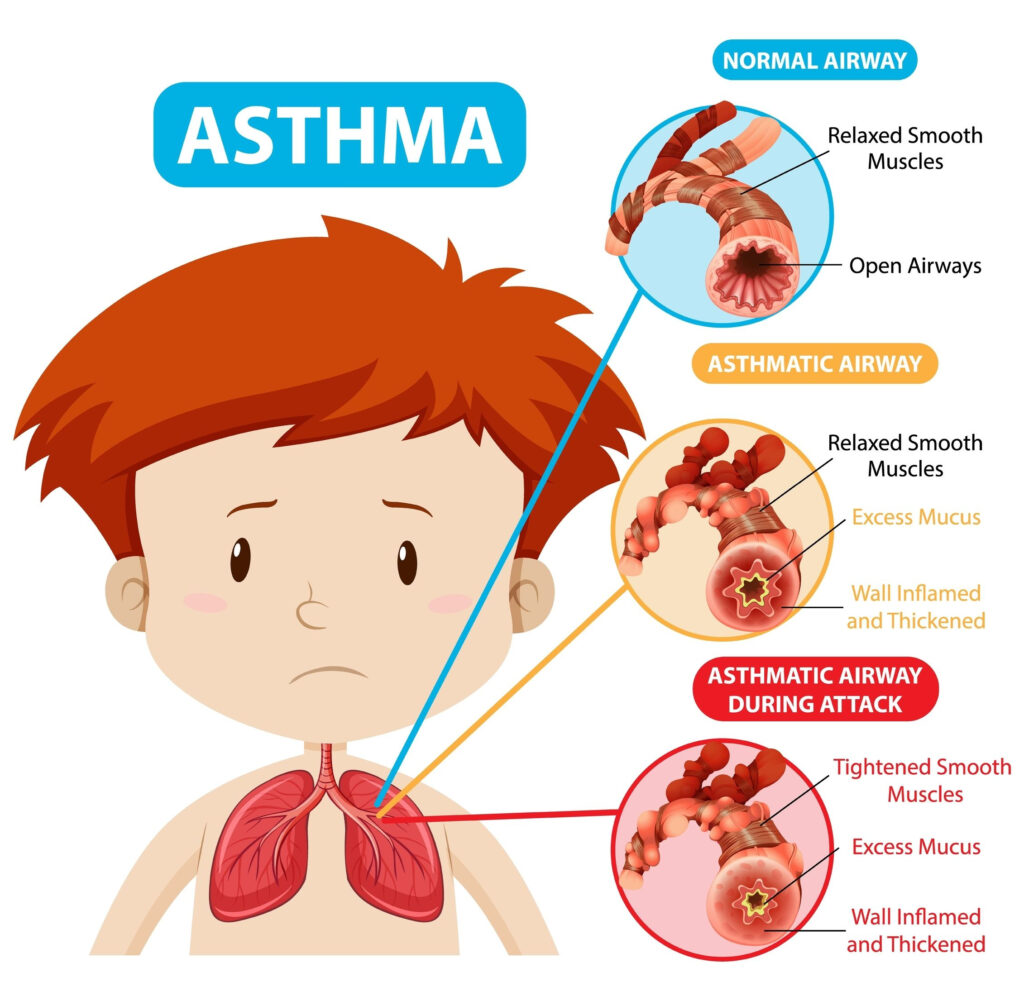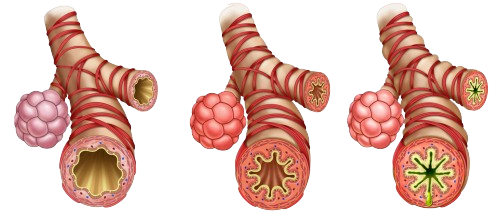


Inflammed, Narrow, Swollen Airways
Genetic, Environment (Pets, Dust, cold, dry air, & smoke), exercise-induced, cold windy weather, cockroaches, Aspirin, NSAIDs such as ibuprofein, ACE inhibitors, Non-selective beta blockers such as propanolol & GERD.
Dyspnea, Wheezing, tachypnea, chest tightness, coughing, anxiety, mucus, air trapping (retaining CO2).

Long-Acting Beta 2 Agonist. E.g., Salmeterol
Beta2 agonist used for rescue. E.g., Albuterol


Prednisone (oral) & Beclomethasone, Fluticasone, Budesonide (inhaled)
Ipratropium Bromide

Montelukast
Blocks immunoglobulin IgE. Given subQ in poorly controlled asthma
Cromolyn. Side effects: temporary burning sensation, teary eyes, sneezing, bad taste mouth.
Ipratropium Bromide
Nursing Care: #1 AIRWAY, Rescue inhaler (Albuterol), Oxygen, High fowler’s, rest to ↓ stress, & assess for signs and symptoms of hypoxia and respiratory failure.
Status Asthmaticus: Emergency, Oxygen, nebulizer medications, IV corticosteroids, & hydration.
| Asthma Type | Frequency of Symptoms |
|---|---|
| Mild Intermittent Asthma | Symptoms occur 2x/week or less |
| Mild Persistent Asthma | Symptoms occur more than 2x/week |
| Moderate Persistent Asthma | Daily symptoms with exacerbations 2x/week |
| Severe Persistent Asthma | Constant symptoms and frequent exacerbations |
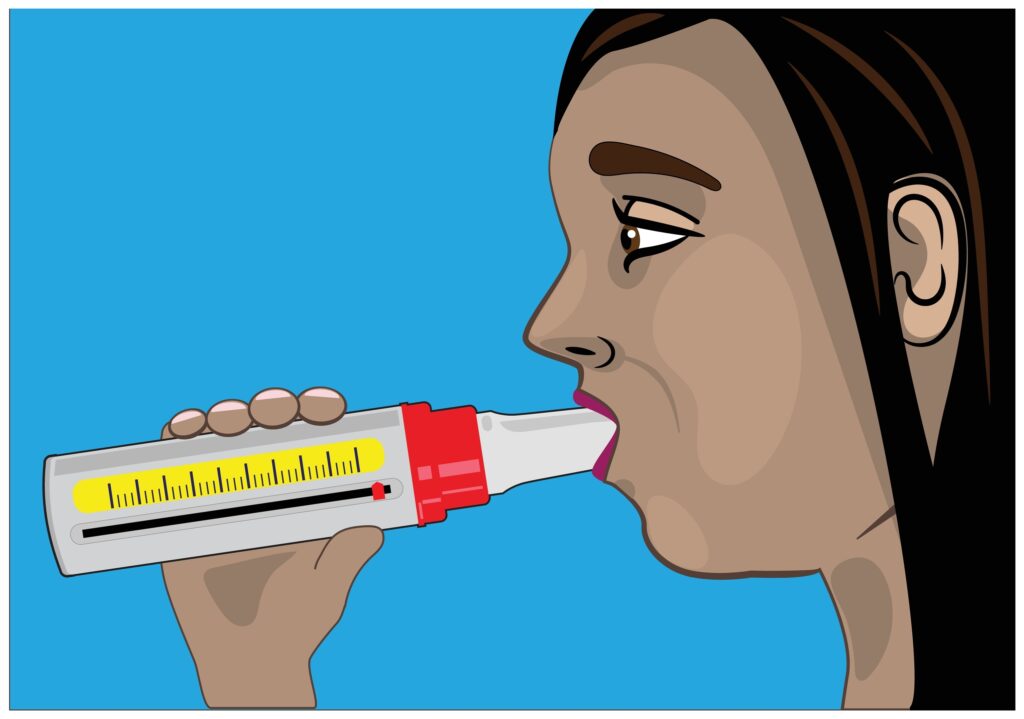
The “personal or usual best” peak flow is the highest number a client can perform over a two-week period when asthma is under good control. Good control means the client feels good and does not have any symptoms. The client then will compare all of other peak flow readings to his or her personal best peak flow number.
To find a personal best peak flow:
Early Warnings of an asthma attack
Active asthma attack that requires intervention