The endotracheal tube used for mechanical ventilation
Airway
It is used to maintain patent airway. Patent airway is always the #1 priority.
Vocal Cords
If a client still needs an ET tube (needs mechanical ventilation) more than 10-14 days, a tracheostomy is performed. Why? Protect vocal cords.
X-Ray
Confirm ET tube placement with a chest xray. Priority after intubation? Get a chest xray!
Cuff Pressure
ET tube cuff pressure should be checked every 8 hours and should be < 20 mm Hg.
Problems
Stomach intubation: breath sounds over stomach. ET Tube in right main bronchus = no breath sounds on the left side because ET tube is in the right side of lung.
Anyways, remember that when suctioning, you must insert suction catheter withOUT suction and apply suction as you remove catheter. Suction regulator should be set at 120-140 mm Hg. Suction < 10-15 seconds. NCLEX Alert
Can you see the endotracheal tube?
Preventing Ventilator-Associated Pneumonia
Sedation Vacation
Assess client’s readiness for extubation/ extubate as soon as possible.
Positioning
Keep the head of the bed elevated 30 to 45 degrees. Reposition client
Suctioning
Suction oral and pharyngeal secretions and provide oral care every 2 hours
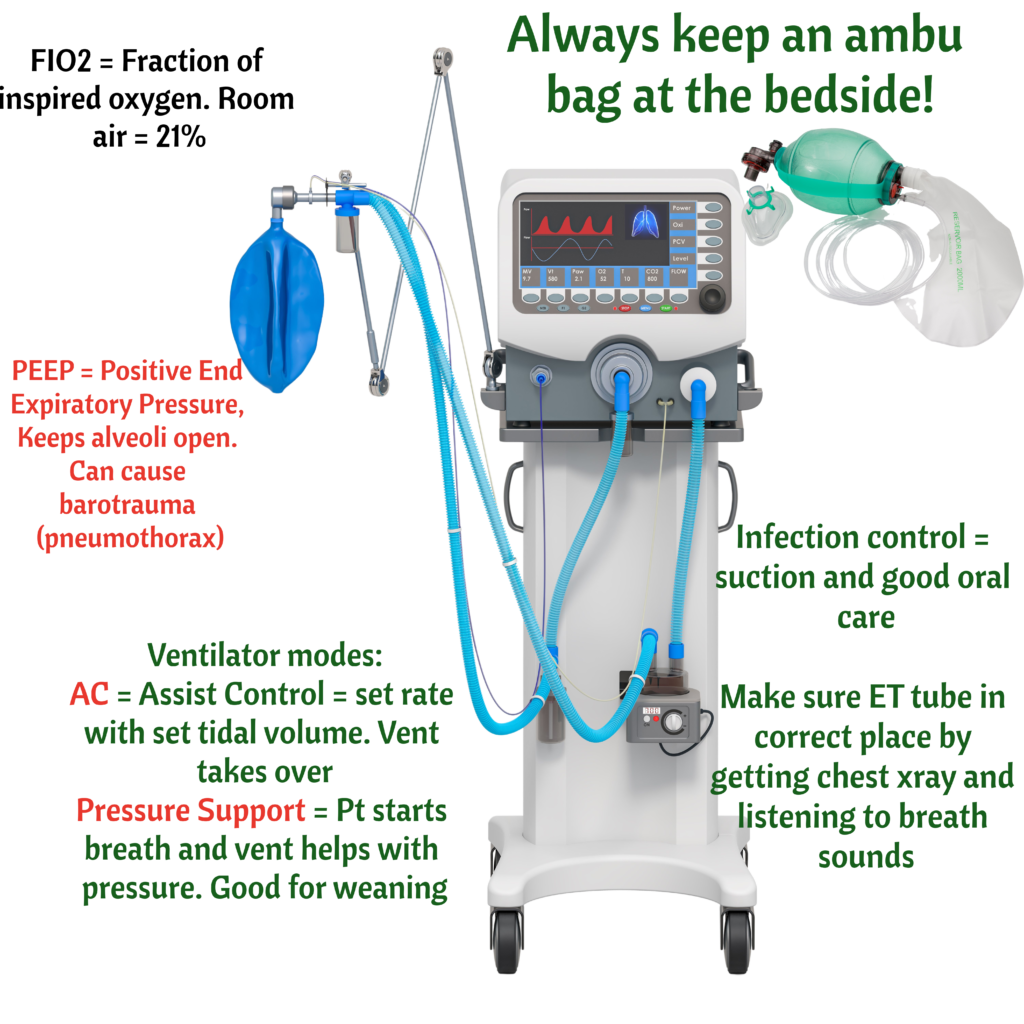
It the tubing becomes disconnected = LOW PRESSURE ALARM. Makes sense, ventilator working against no pressure
If there is an obstruction, lots of water in the tubing, or client has lots of secretions = HIGH PRESSURE ALARM. Makes sense, ventilator working against resistance/pressure.
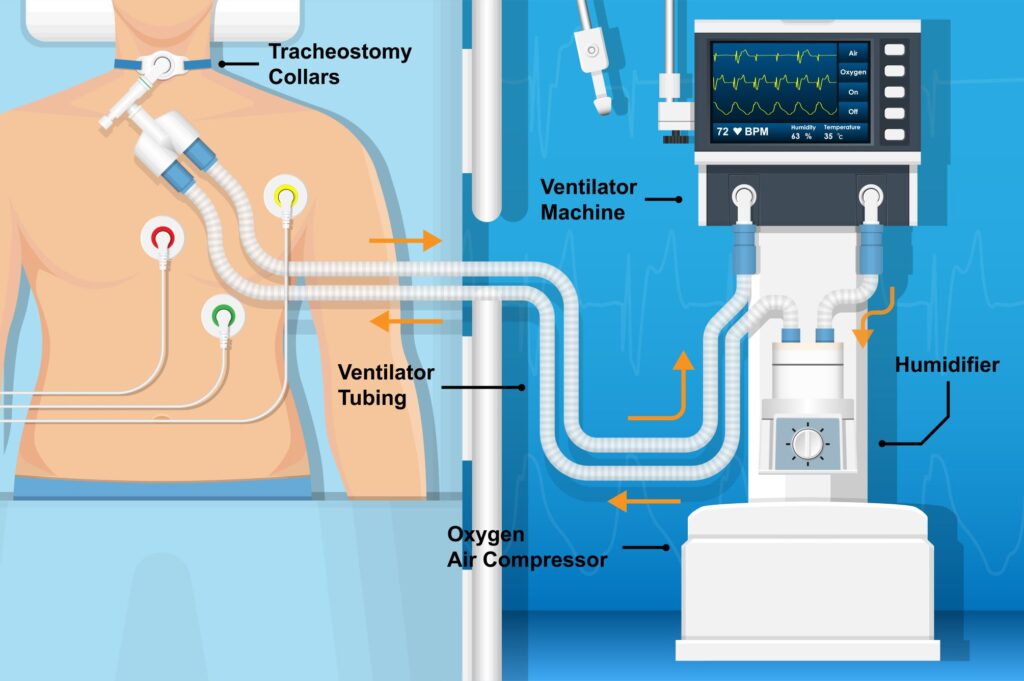
Remember that ventilators use humidified air which condenses into water.
Finally, if the ventilator is going off and you have no idea what is happening, the answer both on the NCLEX and in practice is to check the client. Look at the client. Never troubleshoot any equipment without looking/assessing the client. AMBU BAG the client. Repeat after me, AMBU BAG, AMBU BAG (ahh, and make sure ambu bag is connected to oxygen)
Fast rate (⇑ Respiratory rate) and increased tidal volume blow off more CO2 leading to HYPERVENTILATION or decreased pCO2.
Here is a hyperventilation ABG: pH 7.52, PCO2 30, HCO3 22. Respiratory alkalosis! Yes, Hyperventilation = low pCO2 = respiratory alkalosis
Hypoventilation = low rate and/or low tidal volume, leading to high pCO2. Here is a hypoventilation ABG: pH 7.32, PCO2 55, HCO3 23. Respiratory acidosis! Retaining pCO2
Ready! To get rid of pCO2, you either breathe faster or breathe deeper.
Tidal volume is a measure of the amount of air a person inhales during a normal breath