
Priority Action: What should the nurse do first?



What to do first if this happens.
Place client in left Trendelenberg. Left side with head lowered
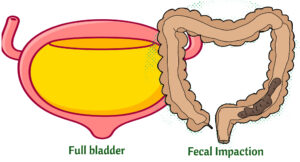
Sit up in bed to decrease blood pressure. Check for bladder distension or fecal impaction. Remove any noxious stimuli.
Autonomic Dysreflexia is an overactive autonomic system in which the client experiences severe hypertension and bradycardia. It is usually due to a spinal cord injury.
- Oxygen and Morphine always show up as choices. But you may also see nitroglycerin and aspirin.
- Remember MONA- morphine, oxygen, nitroglyceirn and aspirin
- Goal: Treat chest pain. Chest pain = myocardial ischemia/infarct
Assess for muscle weakness and check potassium levels.
Check potassium levels and digoxin levels. Hypokalemia potentiates digoxin toxicity. If a client has visual disturbances (e.g., seeing halos) and GI symptoms such as diarrhea always think digoxin toxicity. Normal digoxin level is 0.8- 2.0 ng/mL
Too much antidiuretic hormone. Client retains fluid. Client is hyponatremic (dilution from too much fluid). Priority is to restrict fluids
Have the external/transcutaneous pacemaker at the bedside
Priority is to stop the infusion.
Report black-colored stools= GI bleeding
Priority is to check breathing. Remember that paralysis/weakness starts from the lower extremities and moves up the body. The client will go into respiratory arrest/distress as the breathing muscles become weaker/paralyzed.
Don’t do any activity that would further decompensate client such as getting the client out of bed. Keep unstable clients in bed. Also, never feed a client who is having trouble breathing.
Check Blood sugar
Get intubation tray. Any client in respiratory distress, get ready to intubate is almost always the answer.
- Watch for nephrotoxic drugs/antibiotics/Contrast dye
- Watch for electrolyte imbalances, especially hyperkalemia
- Have tracheostomy tray at the bedside in case of airway closure due postoperative edema/bleeding/hematoma
- Check for hypocalcemia, even in thyroidectomies. The parathyroid may have been damaged during surgery.
- Two important signs of hypocalcemia: Chvostek’s and Trousseau’s sign. And also numbness and tingling.