Adult Nursing NCLEX Review
NCLEX fast Diagnostic NEW
Disaster Triage, Prioritizing, and Delegation
4 Topics
|
2 Quizzes
Prioritizing: Who is the priority client?
Priority Action: What should the nurse do first?
Delegation
Emergency Triage
Prioritizing NCLEX-like Critical Thinking Questions
Delegation NCLEX-like Critical Thinking Questions
Neurological System
10 Topics
|
1 Quiz
Neurovascular Assessment
Stroke
Meningitis
Alzheimer’s and Delirium
Brain Injuries
Spinal Cord Injury
Seizures
Parkinson’s Disease
Diagnostic Tests
Fast Questions
Neurological NCLEX-like Critical Thinking Questions
MS, MG, and Guillain Barré
4 Topics
|
1 Quiz
Multiple Sclerosis
Myasthenia Gravis
Guillain Barré
Fast Questions and Case Study
MS, MG, & GB NCLEX-like Critical Thinking Questions
The Cardiovascular System
12 Topics
|
1 Quiz
Hypertension
MI & Angina
CHF
Aneurysms
EKG Rhythms
Peripheral Vascular Disease
Deep Vein Thrombosis
Pacemakers
Simple Hemodynamics
Rheumatic Heart Disease
Some Important Cardiovascular Assessments
Flashcards and Fast Questions
Cardiovascular System and NCLEX-like Critical Thinking Questions
Pulmonary System
10 Topics
|
1 Quiz
ABGs
Asthma
Pulmonary Embolism
Pneumonia
COPD & Emphysema
Cystic Fibrosis
Tuberculosis
Mechanical Ventilation & Oxygen Delivery
Chest Tubes
Fast Questions
Pulmonary System NCLEX-like Critical Thinking Questions
Cushing Versus Addison Disease
3 Topics
|
1 Quiz
Addison Disease
Cushing Disease
Fast Questions and Case Studies
Cushing/Addison NCLEX-like Critical Thinking Questions
Thyroid Disorders
2 Topics
|
1 Quiz
Hyperthyroidism vs. Hypothyroidism
Fast Questions and Case Study
Thyroid Disorders NCLEX-like Critical Thinking Questions
Parathyroid Disorders
3 Topics
|
1 Quiz
Hypoparathyroidism
Hyperparathyroidism
Fast Questions
The Parathyroid NCLEX-like Critical Thinking Questions
DI and SIADH
3 Topics
|
1 Quiz
Diabetes Insipidus
Syndrome of Inappropriate AntiDiuretic Hormone
Fast-Knowledge Questions
DI and SIADH NCLEX-like Critical Thinking Questions
Diabetes
10 Topics
|
1 Quiz
Diabetes Type 1
Diabetes Type 2
Diagnosing Diabetes
The different types of Insulin
Insulin Complications
DKA vs HHNS
Hypoglycemia vs Hyperglycemia
Long Term Diabetes Complications
Foot Care
Fast Questions and Case Study
Diabetes NCLEX-like Critical Thinking Questions
Burns
5 Topics
|
1 Quiz
Types of Burns
Phases of Burn Management
Rule of 9’s
Complications
Fast Questions
Burns NCLEX-like Critical Thinking Questions
Anemias, Aplastic Anemia, Polycythemia Vera, Thrombocytopenia and DIC
9 Topics
|
1 Quiz
Iron Deficiency Anemia
Pernicious/Megaloplastic Anemia
Folic Acid Deficiency
Aplastic Anemia
Sickle Cell Anemia
Polycythemia Vera
Thrombocytopenia
DIC
Questions
Anemias and more NCLEX-like Critical Thinking Questions
Cancer, Chemotherapy, Radiation Therapy, and Oncological Emergencies
6 Topics
|
1 Quiz
Cancer and Prevention
Types of Cancer
Chemotherapy
Radiation Therapy
Oncological Emergencies
Case Study and Fast Questions
Cancer, Chemotherapy and Radiation NCLEX-like Critical Thinking Questions
Leukemias, Hodgkin’s Disease, and Multiple Myeloma
4 Topics
|
1 Quiz
Leukemias
Hodgkin’s and Non-Hodgkin’s Disease
Multiple Myeloma
Check your Knowledge
Leukemias, Hodgkin’s Lymphoma, and Multiple Myeloma NCLEX-like Critical Thinking Questions
The GI system
16 Topics
|
1 Quiz
Hiatal Hernia
Ulcerative Colitis and Crohn’s Disease
Liver Cirrhosis
Pancreatitis
Hepatitis
Celiac Disease
Colostomies
Esophagogastroduodenoscopy
Dumping Syndrome
Diverticulitis
Cholecystitis
Appendicitis
Peptic Ulcers
Tube Feedings
GI Flashcards
Fast Questions
GI System NCLEX-like Critical Thinking Questions
Renal and Genitourinary Problems
6 Topics
|
1 Quiz
Functions of the Kidney
Acute and Chronic Renal Failure
Glomerulonephritis
Urinary Tract Infection
Benign Prostatic Hyperplasia
Hemodialysis and Peritoneal Dialysis
Renal and GU Problems NCLEX-like Critical Thinking Questions
Infection and Isolation Precautions
3 Topics
|
1 Quiz
HIV
Some STIs you should know
Isolation Precautions
Infection NCLEX-like Critical Thinking Questions
NCLEX Pharmacology
3 Topics
|
1 Quiz
NCLEX Must-Knows
FlashCards
Classes of Drugs
NCLEX-like Pharmacology Questions
Famous Antidotes & Therapeutic Levels
Famous Drugs, Safety Precautions, Signs & Symptoms, Clinical Signs and Pressure Sores
6 Topics
Famous Drugs
Famous Safety Precautions
Famous Signs and Symptoms
Famous Clinical Signs
Famous Mnemonics
Pressure Sores
Famous Procedures, Positions, Diets, and Assessments
4 Topics
Procedures
Positions
Diets
Assessments
TPN, IV Solutions, & Blood Products
6 Topics
|
1 Quiz
TPN
IV Solutions
Blood Products
Blood Products Flash Cards
IVs and Central Lines
Fast Questions
IV’s, TPN, & Blood NCLEX-like Critical Thinking Questions
Lab Values
9 Topics
About Lab Values
Sodium
Potassium
Calcium
Phosphorus
Magnesium
NCLEX Questions
More Labs that you should know
Flashcards!
Critical Care Lessons
Learning Activity
Study commonly tested material using flashcards
Questions
Previous Lesson
Next Topic
TPN
Adult Nursing NCLEX Review
TPN, IV Solutions, & Blood Products
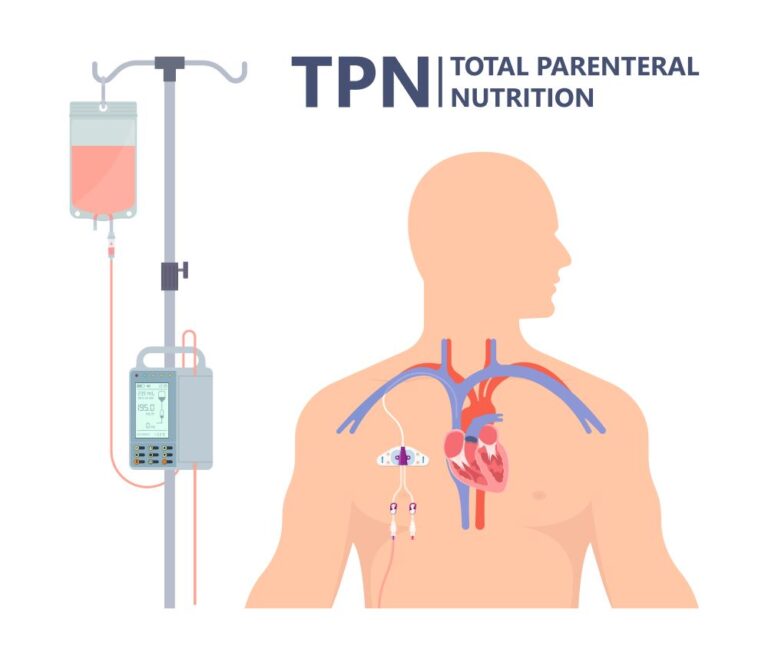
TPN
Total Parenteral Nutrition
Dysfunctional GI tract
GI surgery
Intolerance to tube feedings
Malnutrition from burns, cancer, or chemotherapy
Least desirable form of nutrition. Only used when it is the only choice.
Indications
Administration
Administered via central line, peripherally inserted central catheter, or implanted vascular access
Hypertonic (high concentration of solutes and glucose > 15%
Composition
Glucose concentrations varies from 5% to 70%.
Amino acids
Lipids
Vitamins
Electrolytes
Insulin to counteract high glucose content.
Aseptic Techniquen when changing central line dressing and hanging new TPN. Monitor signs and symptoms of infection.
Nursing Interventions
Never stop TPN abruptly, wean down.
Once discontinued check blood sugar 1 hour after.
Weight patient daily
Never increase rate for “catch up”
Monitor I & O
Aseptic Technique when changing TPN
Hang D10W if you run out of TPN
Monitor glucose every 4 hours with insulin sliding scale
Monitor Electrolytes
Return cloudy/dark solution
Must be hung within 24 hours of preparation by pharmacy
Complications
Fluid overload: hypertension, edema, dyspnea, crackles. Elevate HOB. Reduce rate per MD order
Pneumothorax from incorrect catheter placement. Make sure an x-ray is done for correct placement.
Infection: Monitor for fever, chills, nausea, vomiting, redness and swelling at insertion site
Air embolism: Air enters vein through tubing. Clamp tubing and turn patient left trendelenburg position
Peripheral Parenteral Nutrition
Given through a peripheral IV
Low glucose concentration (< 12.5% glycose)
Used for short term (5 to 7 days)
Used when client needs smaller concentration of carbs, fats, and proteins
PPN delivers isotonic or midly hypertonic solutions since highly hypertonic solutions can cause sclerosis, phlebitis, or swelling to peripheral veins.
Previous Lesson
Back to Lesson
Next Topic
Review Your Cart
0
Discount
Add Coupon Code
Apply
Subtotal
Total Installment Payments
Bundle Discount
Checkout
0
Login
Accessing this course requires a login. Please enter your credentials below!
Username or Email Address
Password
Remember Me
Lost Your Password?
Register
Don't have an account? Register one!
Register an Account