Patient education should focus on recognizing risk factors and managing modifiable risks
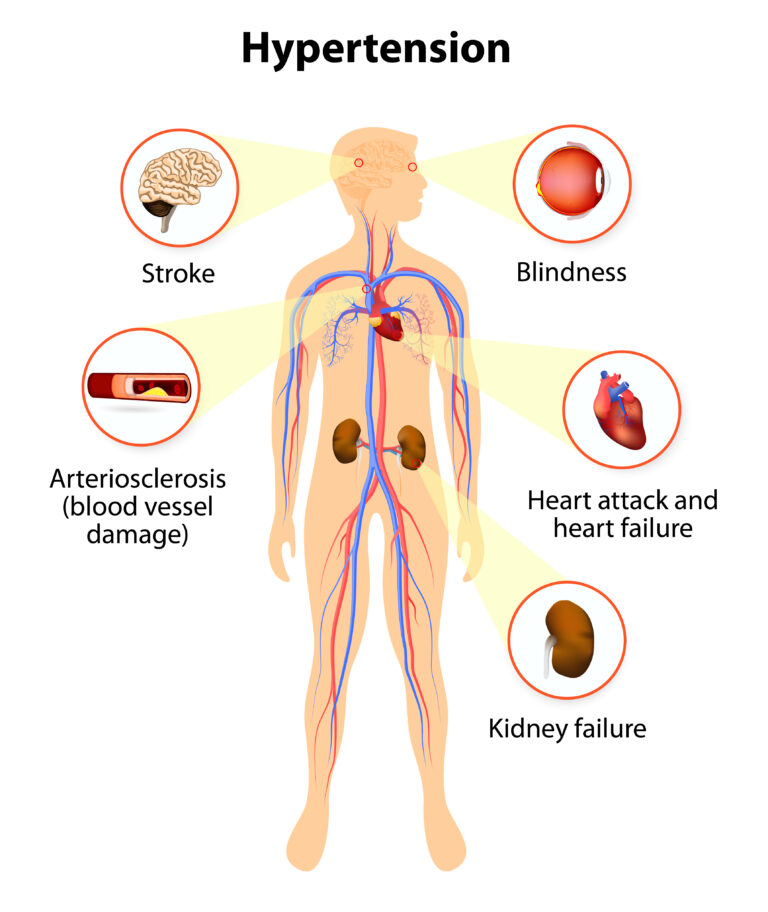
Hypertension is a modifiable risk for coronary artery disease and stroke. Also modifiable is cigarette smoking, and hyperlipidemia.
How to modify them:
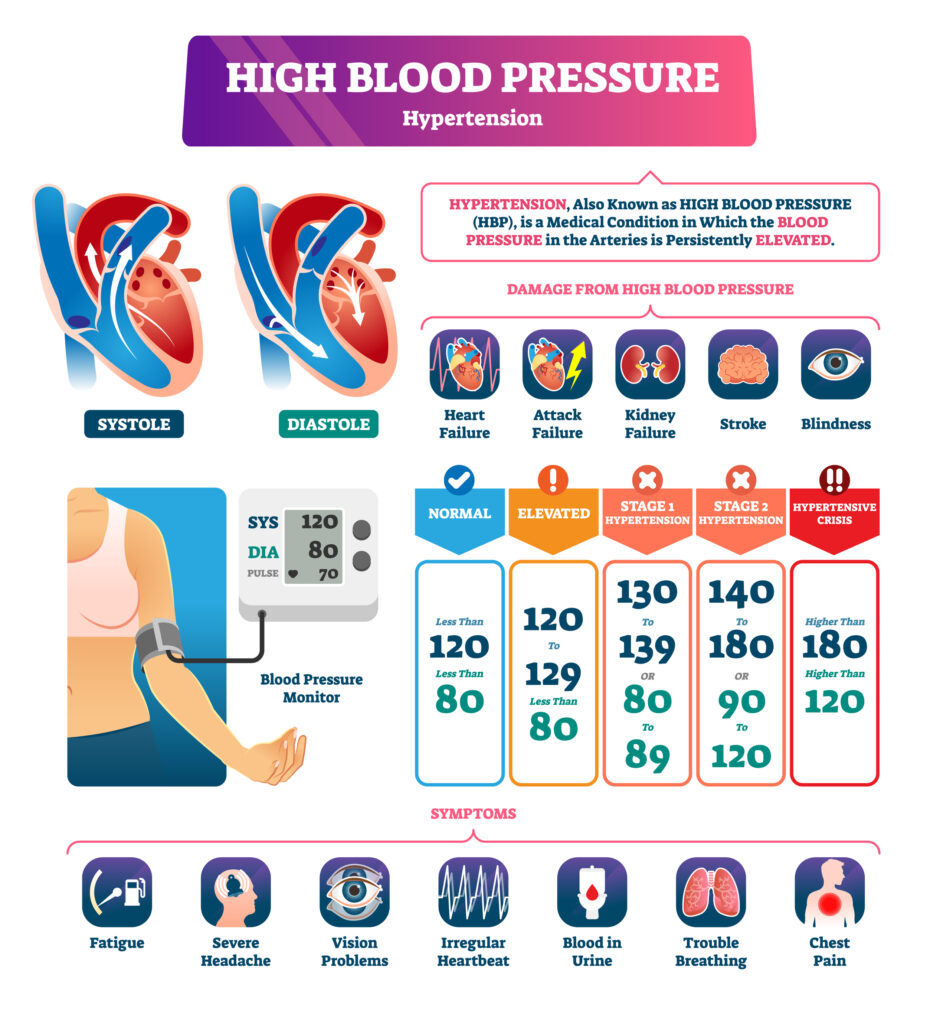
Hypertension: control BP with meds/exercise/diet
Smoking: Stop
Hyperlipidemia: exercise/diet/meds
Ok, diabetes can also lead to CAD/Stroke/kidney disease. Diabetes can also be controlled.
Non-modifiable: Age, genetics, and ethnicity.
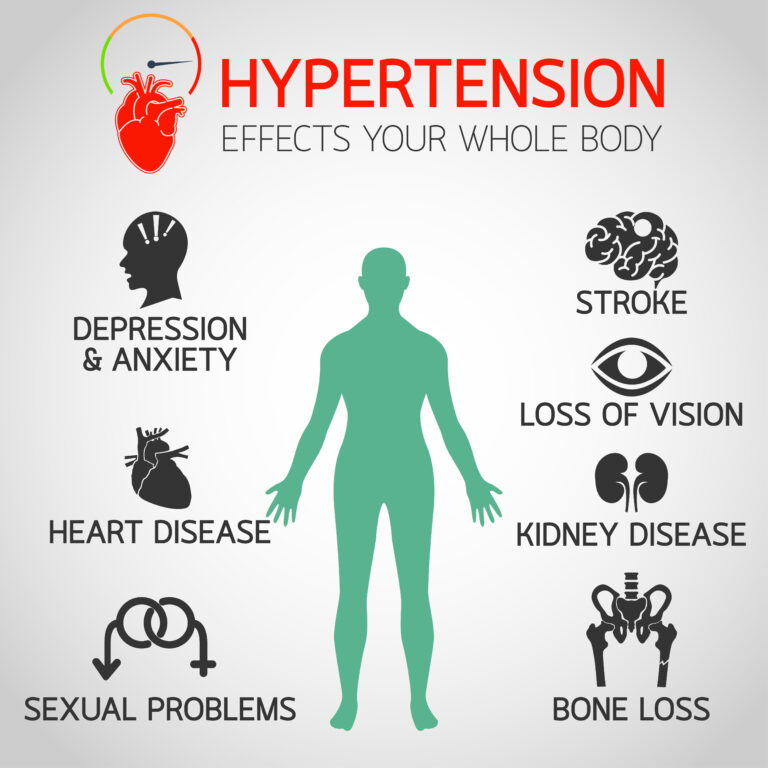
Bone loss? In hypertension patients, excess urinary calcium secretion induces secondary parathyroidism to increase serum calcium level by calcium release from bone, which may accelerate osteoporosis.
Patient education
Low-sodium diet. Not moderate. LOW
Watch out: Salts substitutes have potassium. If the patient has kidney disease or is taking ACE inhibitors, that’s a problem. Patient may be taking salt substitutes to stick with low sodium diet, but now they will have hyperkalemia.
Home monitoring of BP at least once weekly.
Goal BP <140/90
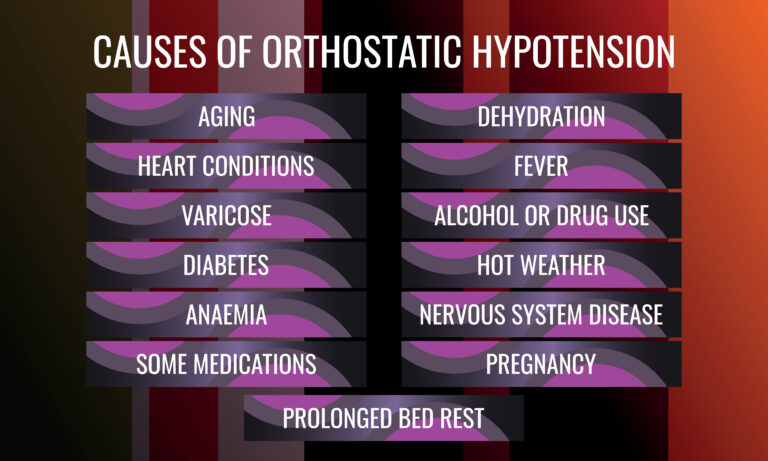
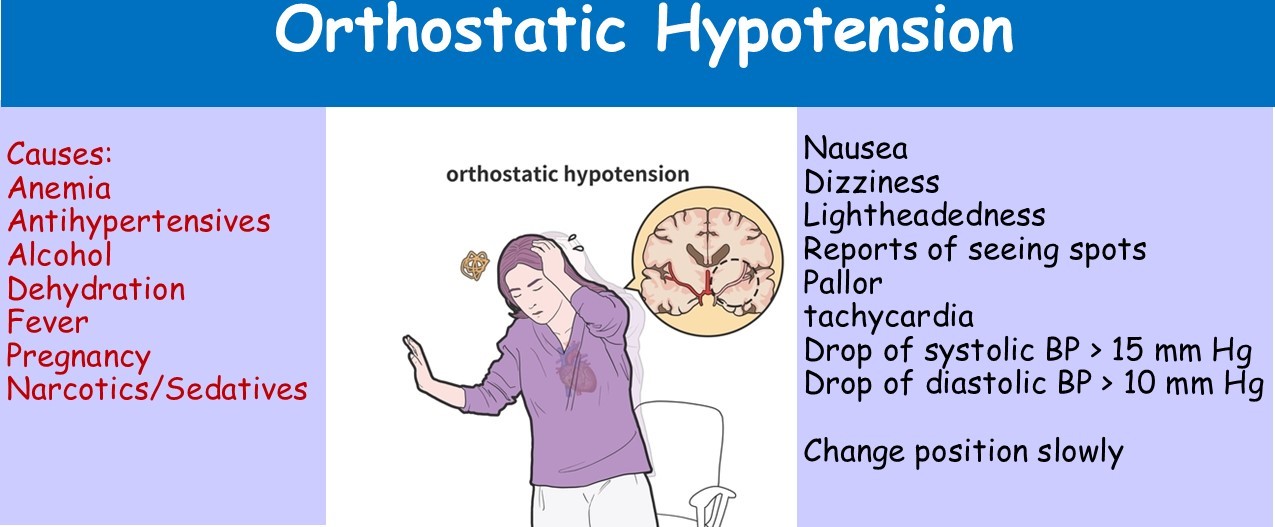
Orhtostatic Hypotension. Most if not all, antihypertensives cause orthostatic hypotension. Change position slowly. Let me say that again. Ok, I won’t. Just read it again.
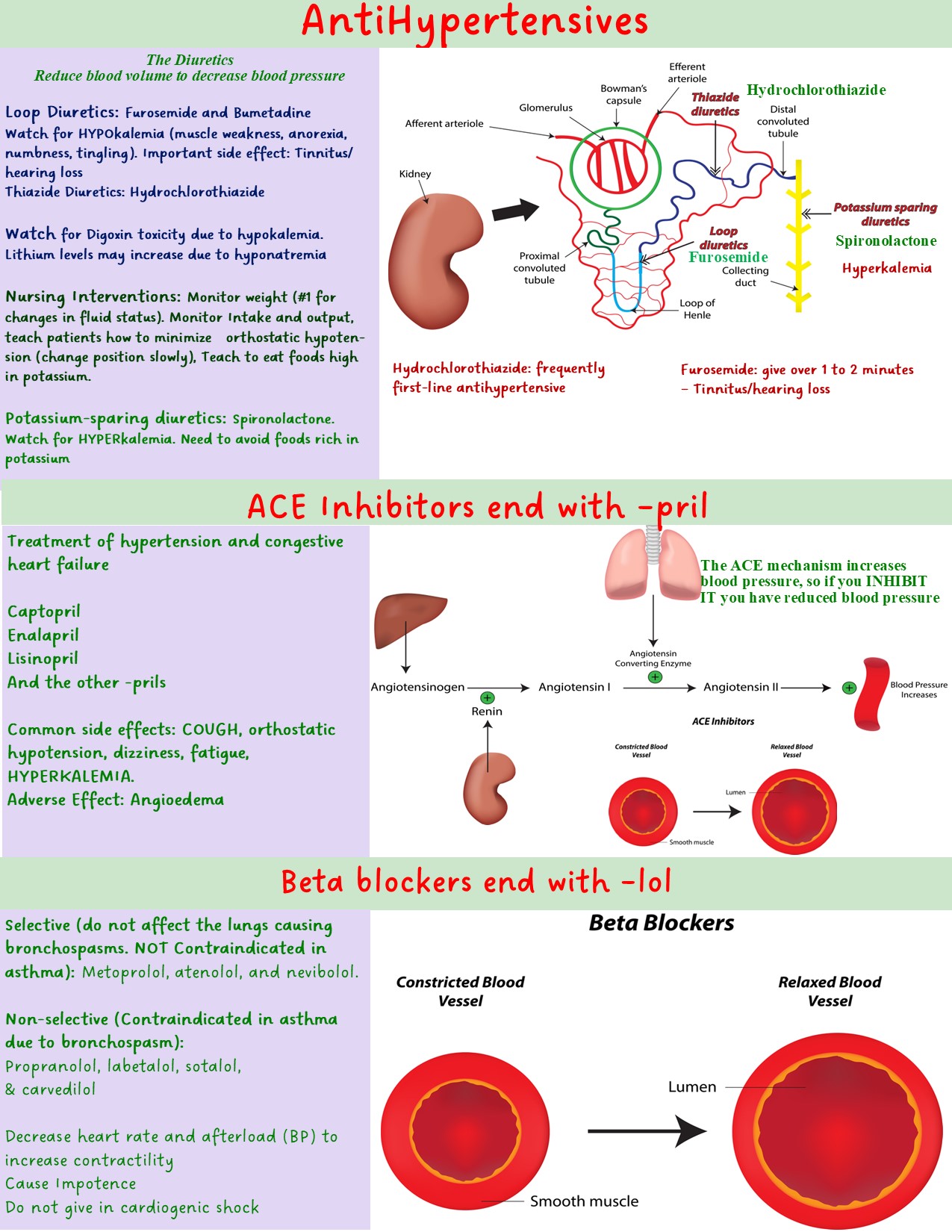
Hypertension causes erectile dysfunction. Beta blockers (metoprolol and the other -lol meds) also cause erectile dysfunction. Compliance with beta blockers is a problem due to erectile dysfunction. So both the disease and the treatment let you down.
What has sodium: Canned foods, crackers, frozen pizza.
Low sodium: stick with fruits and vegetables.,
Test your knowledge
Since antihypertensives cause orthostatic hypotension, let's learn about it