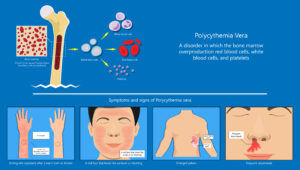
Polycythemia Vera
/*! elementor – v3.12.1 – 02-04-2023 */
.elementor-heading-title{padding:0;margin:0;line-height:1}.elementor-widget-heading .elementor-heading-title[class*=elementor-size-]>a{color:inherit;font-size:inherit;line-height:inherit}.elementor-widget-heading .elementor-heading-title.elementor-size-small{font-size:15px}.elementor-widget-heading .elementor-heading-title.elementor-size-medium{font-size:19px}.elementor-widget-heading .elementor-heading-title.elementor-size-large{font-size:29px}.elementor-widget-heading .elementor-heading-title.elementor-size-xl{font-size:39px}.elementor-widget-heading .elementor-heading-title.elementor-size-xxl{font-size:59px}
The Opposite of Anemia: Polycythemia Vera
/*! elementor – v3.12.1 – 02-04-2023 */
.elementor-accordion{text-align:left}.elementor-accordion .elementor-accordion-item{border:1px solid #d5d8dc}.elementor-accordion .elementor-accordion-item+.elementor-accordion-item{border-top:none}.elementor-accordion .elementor-tab-title{margin:0;padding:15px 20px;font-weight:700;line-height:1;cursor:pointer;outline:none}.elementor-accordion .elementor-tab-title .elementor-accordion-icon{display:inline-block;width:1.5em}.elementor-accordion .elementor-tab-title .elementor-accordion-icon svg{width:1em;height:1em}.elementor-accordion .elementor-tab-title .elementor-accordion-icon.elementor-accordion-icon-right{float:right;text-align:right}.elementor-accordion .elementor-tab-title .elementor-accordion-icon.elementor-accordion-icon-left{float:left;text-align:left}.elementor-accordion .elementor-tab-title .elementor-accordion-icon .elementor-accordion-icon-closed{display:block}.elementor-accordion .elementor-tab-title .elementor-accordion-icon .elementor-accordion-icon-opened,.elementor-accordion .elementor-tab-title.elementor-active .elementor-accordion-icon-closed{display:none}.elementor-accordion .elementor-tab-title.elementor-active .elementor-accordion-icon-opened{display:block}.elementor-accordion .elementor-tab-content{display:none;padding:15px 20px;border-top:1px solid #d5d8dc}@media (max-width:767px){.elementor-accordion .elementor-tab-title{padding:12px 15px}.elementor-accordion .elementor-tab-title .elementor-accordion-icon{width:1.2em}.elementor-accordion .elementor-tab-content{padding:7px 15px}}.e-con-inner>.elementor-widget-accordion,.e-con>.elementor-widget-accordion{width:var(–container-widget-width);–flex-grow:var(–container-widget-flex-grow)}
Patho
- ⇑ WBC
- ⇑ RBC
- ⇑ Platelets
- Clients are prone to clots and do not live very long. Die from a myocardial infarct or a stroke.
- Cause: cancer usually in older adults 50- 75 y/o
- Too many RBCs leading to increased hematocrit, hypervolemia, hyperviscosity, and hypertension
- Clients with COPD who have chronic hypoxia may start making for RBCs to compensate.
- Red face due to excess RBCs
- Purple or cyanotic skin and mucuous membranes due to hypoxic blood
- Severe burning/itching due to thick, poorly oxygentated blood.
- Hypertension (remember blood is thick)
- Dilated vessels
- Clots due to obstructed blood flow.
- Infarcts of organs (heart, brain)
- Visual disturbances, headache, orthopnea, gout!
- gout: painful swollen joints (usually big toe)
- Orthopnea is due to heart failure
- dizziness, feelilng of fullness in the head, Tinnitus
- Think hypertension s/s
- Uric acid and potassium increase (gout, renal failure, hyperkalemia)
- Apheresis/phlebotomy: removal of RBCs to reduce viscosity.
- Hydration to reduce viscosity
- No iron supplements
- Anticoagulations (makes sense since at risk for clots)