Problems that have PRIORITY
Let's learn how to prioritize
There is a quiz at the very end of this lesson, so attention
- To determine who is the sickest client, the NCLEX prioritizing questions follow formats similar to these:
- There is an emergency situation, which client should the nurse assess FIRST?
- At the beginning of the shift the nurse gets report on 4 clients, which client should the nurse see FIRST?
- The home health/community nurse is visiting 4 clients today, which client should the nurse visit FIRST?
- The charge nurse is making assignments for the day, which client should the charge nurse assign to the experienced Registered Nurse?
- To determine who is the stable client or who is not as sick, the formats may be as follows:
- The unit is full, which client can be discharged?
- Which client should the charge nurse assign to a new graduate nurse/an LVN/a float nurse/ a travel nurse.

To save reading time and give you more time to learn, the questions provided in this module have been simplified; unless, of course, more background information is needed to understand the question. For example, the questions only ready: “Which client should the nurse assess FIRST?”
Think ABC in that order at all times.
If ABC is not helping you to determine which patient has priority, then think: Is the problem with the patient expected of the disease/problem or is it unexpected/a complication of the problem. The EXPECTED or EXPECTED strategy will be covered after we do ABC.


Again, Prioritizing is about training your mind to think ABC
Airway is always first priority! Here are some airways problems
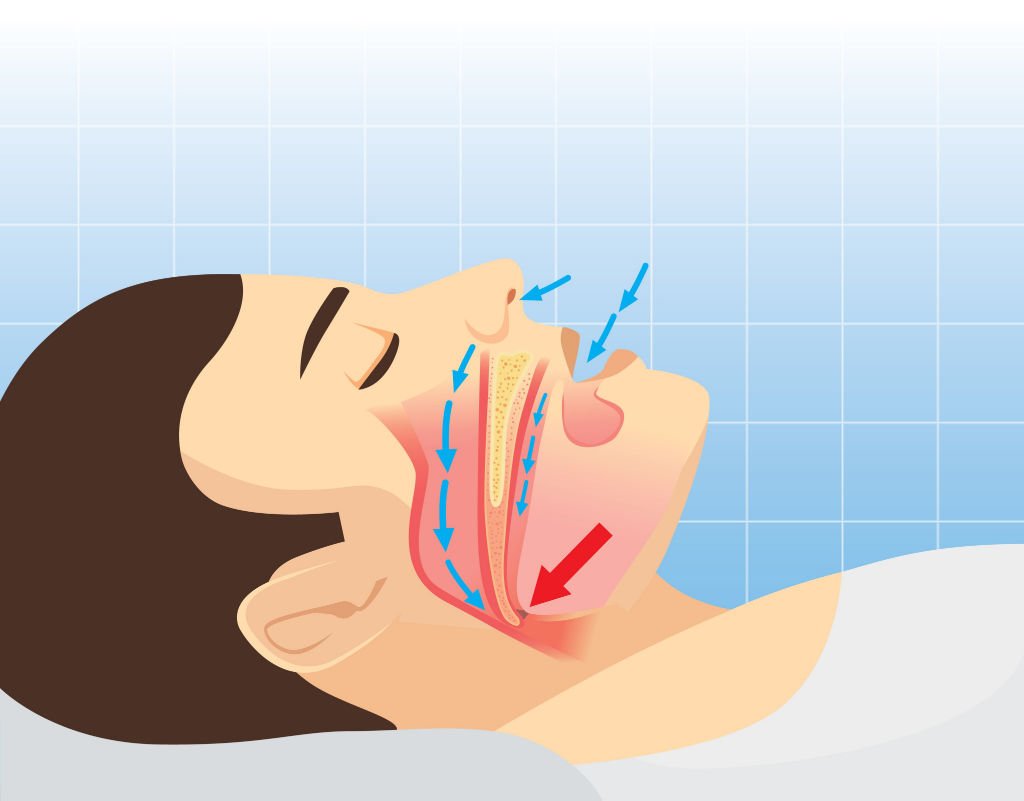
Obstructed Airway (Tongue # 1 Obstruction. Mmm Seizures)
Choking (coughing w/ meals?) Is the patient aspirating?

Drooling= Epiglottitis, especially in kids. Epigottis swells and occludes airway
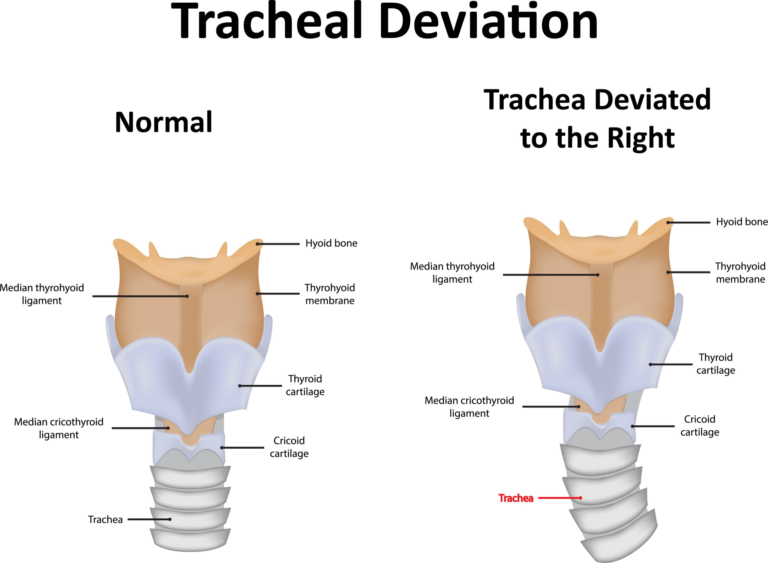
Tracheal Deviation, especially in trauma. Pneumothorax or hemothorax?
Post-thyroidectomy. Think airway swelling, hematoma, & bleeding

Post-Parathyroidectomy. Think hematoma, airway swelling, & bleeding
Anaphylactic Shock/Allergic reaction=Airway swelling

Stridor=Air can't get through due to swelling. Ok, noisy breathing is bad, but also diminshed breath sounds is bad. Air not getting through. A patient with an asthma attack who is wheezing is not as bad as a patient with diminished breath sounds.

Smoke Inhalation. Damage to airway?

Face/Beard Burns. Airway mucosa edema?

Seizures and Altered Level of Consciousness (Can't protect airway)
Losing Endotracheal Tube/ Tracheostomy or Ventilator Alarm. If you have an intubated patient and the ventilator alarm is going off, go see that patient. The patient with a fever who you think is septic can wait a few minutes and even the patient with a heart attack can wait a few minutes.
Next in the priority list are breathing problems


Drug Overdose/ ALOC (Not breathing)

Acute Hypoxia/Low Saturations. Remember in COPD mild hypoxia is not ACUTE. A client with COPD may not be the priority client. The NCLEX loves to add that COPD patient with CHRONIC (as you should know) low saturations who is dyspneic because he/she walked to the restroom. You immediately think BREATHING, but this is a chronic hypoxia because ACUTE vs CHRONIC also matters, as we will see later. Think twice before you choose that COPD patient. Are they telling you that the patient is in acute respiratory distress or are the patient's signs and symptoms part of the disease process?Mmmm
Respiratory Acidosis with pCO2 > 60 mm Hg and pH< 7.35
Chest Trauma- Hemothorax
Chest Trauma - Pneumothorax
Neurological Events (Brain controls breathing). Example, a guilllian Barre client with shallow breathing due to respiratory muscle paralysis is priority. That Guillian Barre patient with decreased vital capacity needs you now!
Next in the priority list are CIRCULATION problems


Chest Pain-Myocardial Infarction


Abnormal rhythms with symptoms (dizziness, chest pain, shortness of breath) such as heart blocks/ bradycardia/ tachycardia. And of course, all the deadly rhythms such as ventricular tachycardia, ventricular fibrillation, asystole which require either CPR or ACLS

A malfunctioning Pacemaker. Imagine if the patient's underlying rhythm is a deadly bradycardia and pacemaker is not working. What if the patient is being taken to MRI despite having a pacemaker. Go save him!

Clients described as UNSTABLE due to low blood pressure/ tachycardia/ respiratory distress/ poor peripheral perfusion/cold skin/ diaphoretic/ lethargic/ 1+ pulses

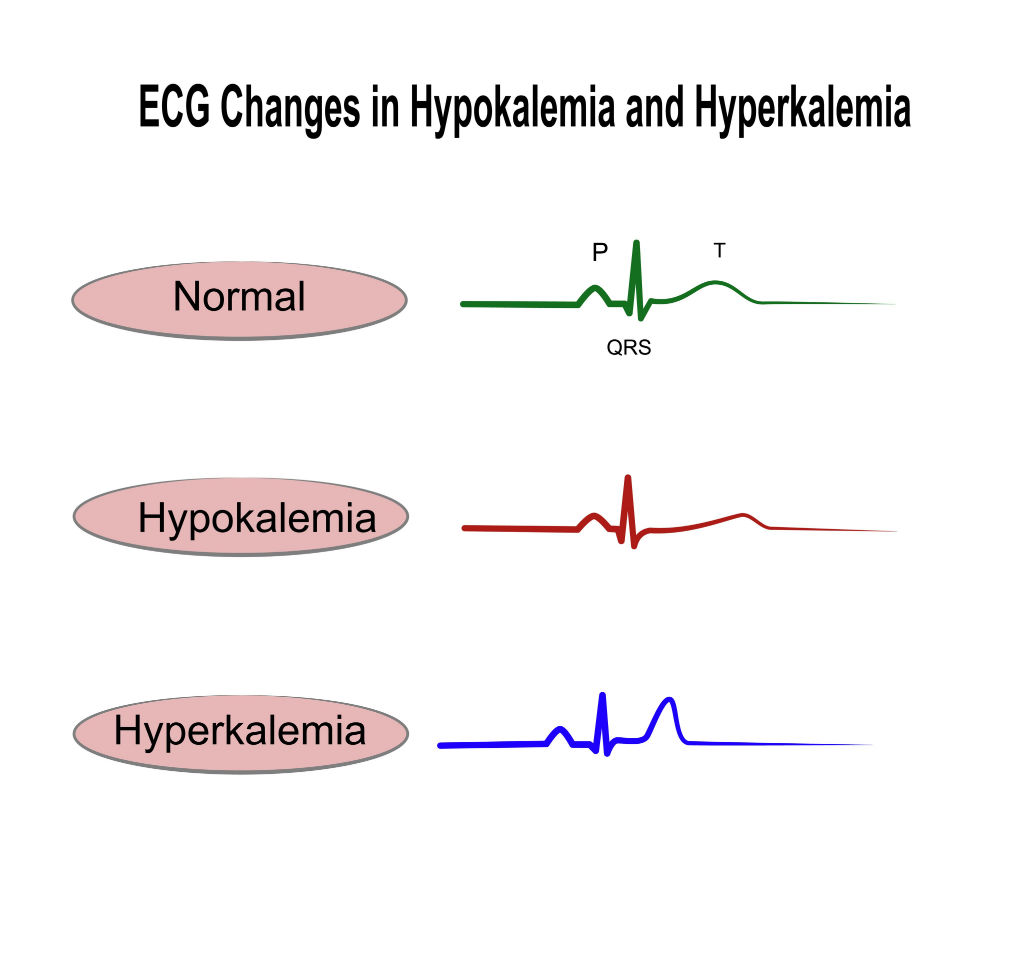
Deadly labs such as hyperkalemia and severe acidosis (Low pH). Since we are here, make sure you know the above EKG changes. Hyperkalemia- tall peaked T wave
Oh, Here I am! Bleeding. Look for postoperative bleeding such as a distended abdomen or a bleeding abdominal aneurysm(=sudden back pain)
Choose ACUTE problems over CHRONIC problems
Let's look beyond ABC in order to answer prioritizing NCLEX questions!

Let's think in terms of EXPECTED versus UNEXPECTED symptoms. UNEXPECTED symptoms are symptoms that signal a potential complication.
UNEXPECTED Symptoms/Complications
- Give priority to clients with unexpected symptoms that are life-threatening or represent a serious complication that compromise ABC.
- Try to answer this question to understand what an expected and an unexpected symptom is.
- Never forget, that yes, all patients need to be seen. All are sick. All need you and you will see all, but which one will die sooner if you don’t see him or her right this minute.
- The client on insulin drip has no life-threatening emergency. Blood sugar is elevated, but the client is receiving treatment. EXPECTED (Hypoglycemia; however, would be a complication of treatment and would have priority).
- Back pain in an abdominal aneurysm= rupture (circulation). UNEXPECTED/COMPLICATION
- Client’s with COPD are expected to have lower saturations and be short of breath with activity. EXPECTED
- The client with pancreatitis is EXPECTED to be in pain.
- Remember: Do not make assumptions. Do not assume that a client with low saturations is in respiratory distress.
NCLEX MUST-KNOW:: Back pain in abdominal aneurym=rupture

- Vomiting in a client with esophageal varices is UNEXPECTED because it’s a sign of a serious complication (RUPTURE/BLEEDING).
- Pain is EXPECTED in sickle cell crisis. It’s important to treat pain, but saving a client who can bleed out is priority.
- Blood in the stool of a client with Crohn’s disease is EXPECTED.
- Client’s with pneumonia (an infection) are EXPECTED to be febrile.
- A client on skeletal traction is EXPECTED to have pain. Please don’t think that maybe pain is due to possible nerve damage, especially when you have a patient with decrease perfusion to the leg.
- A fasting blood sugar of 80 mg/dl is normal. EXPECTED
- Tidaling in the water seal of a chest tube is EXPECTED. Bubbling in the suction chamber is EXPECTED. However, bubbling in the water seal would be UNEXPECTED (=air leak). Unless it is intermittent bubbling after chest tube insertion due to pneumothorax. Memorize these. We will cover chest tubes in the nursing procedure module.
- Decreased pulses after a cardiac cath is UNEXPECTED. It’s a CIRCULATION problem. Notify the physician or the client may lose an extremity. By the way, decreased perfusion to an extremity always comes up. Look for pulses 1+, pale or cool fingers/toes or numbness and tingling.
NCLEX MUST KNOW:: nausea/vomiting in esophageal varices=potential rupture
NCLEX MUST-KNOw::Tidaling in water seal of a chest tube is EXPECTED. Bubbling in the suction chamber EXPECTED. Bubbling in the water seal NOT EXPECTED (=air leak) unless it is intermittent bubbling after chest tube insertion due to pneumothorax. Remember that air needs to come out somehow.
NCLEX MUST-KNOW:: Decreased pulses, numb toes, cool toes after a heart cath is a Priority=damage to arteries.
- A client admitted for dehydration is expected to be a little tachycardic. Please don’t begin to think hypovolemic shock when you have the bleeding patient with a distended abdomen as a better choice. A patient with a heart rate of 102 won’t die if you see him in 15 minutes. EXPECTED
- A client with a bowel resection is not expected to have a fever. UNEXPECTED. But let’s look if there is something with greater priority. A post-op fever can wait a little. Ahhh! Now you are thinking: this expected/unexpected strategy is not perfect or doesn’t work all the time. Nothing is black and white. Here is what critical thinking comes into play.
- A client with a chest tube to suction is EXPECTED to have bubbling in the suction chamber.
- A client with an appendectomy and a distended abdomen likely has post-surgical bleeding. UNEXPECTED. This is a circulatory problem. It has priority over an infection. By the way, make sure you know that BLEEDING/HEMORRHAGE is the number 1 post-surgical priority (of course, unless airway and breathing are compromised). Most people choose pain when asked what is the number 1 post-surgical priority. Be a hero and choose HEMORRHAGE.
- A client with osteomyelitis has an infection. Nausea is often expected.
- Itchiness is common in clients with chronic renal failure due to elevated phosphorus; however, if a client receiving a blood transfusion or medications such as antibiotics is itchy, think potential allergic reaction. This would be a priority client. Stop the blood or antibiotic or whatever patient is getting. That’s the answer on the NCLEX.
- The client with chest pain is potentially having a myocardial infarction. Remember, MI is a priority. Unless you have patient with a compromised airway or not breathing. See them first and then move on to the heart attack.
- A client with chronic renal failure is EXPECTED to be anemic. Usually hospitals do not transfuse unless hemoglobin is < 7.0 mg/dL. There is no mention that the client is symptomatic.
- A client with chronic renal failure is EXPECTED to have an elevated creatinine. FYI, and BUN.
- A client with an infected diabetic ulcer is EXPECTED to have an elevated WBC.
- A potassium of 7.0 mg/dl is hyperkalemia. Hyperkalemia is a deadly lab. It can stop the heart. UNEXPECTED/COMPLICATION. Go save this patient! Please know you normal potassium level (3.5 to 5.5 mEq/L) in order to detect hyperkalemia. Let me tell you, if a choice has a patient with hyperkalemia, I bet you that is your priority patient.
Unstable
- If an answer choice describes the client as UNSTABLE. Think no more…This is likely the PRIORITY client.
- If the “unstable” word is not in the answer choice then what makes a client unstable?
- Hypotension
- ALOC
- Bleeding. Here it is again!
- Abnormal heart rhythms such as heart blocks.
- An abnormal deadly lab such as low blood sugar and hyperkalemia.
- Too obvious, I hope. The word unstable is in the question.
- Let’s try the next one.
- Nausea is a common side effect of most medications, not just hydrocortisone.
- The client with asthma is still having air exchange (the client has wheezes). If the client had decreased breath sounds that means that the client’s respiratory passages are about to close down. The client may go into respiratory arrest. However, wheezes and a respiratory therapist at the bedside is reassuring.
- The hypotensive, tachycardic, difficult-to- arouse client is UNSTABLE. Ok, this question is too obvious. Sorry for that.
ACUTE over chronic
- Simple. Acute problems have priority over chronic problems.
- The client with acute appendicitis has priority over the the client with a myocardial infaction who was admitted 7 days ago and will be discharged the next day.
- The client with acute vomiting has priority over a client with a chronic problem.
- The client with an acute severe headache has priority over a client with chronic obstructive pulmonary disease (even when COPD is respiratory and you were taught “airway” first). A severe headache may be a ruptured cerebral aneurysm! Bleeding or a brain bleed/stroke that may affect ABC!
- The client with an elevated BP has had it for at least a day. Not an acute problem.
- The client who pulled out his NG tube did it 5 hours ago. If it was not a priority 5 hours ago, it is definitely not now.
- The client with sudden chills has an “acute” change in condition. You may say, but wait a minute, we just had a patient with a potential infection, with a fever and that patient was not a priority patient. Well, in that scenario the patient was not priority because someone was sicker, but here, in this question, this patient is the one with an acute change in condition. Critical thinking! So sepsis/infection may not be a priority in some scenarios because there may be a patient with an ABC problem.
Allergic Reactions
- Allergic reactions can vary from simple hives to anaphylaxis (closing of the airway). Prioritize symptoms of allergic reactions.
- And remember if a client is having an allergic reaction during a medication administration or blood transfusion, the first action is to stop the infusion.
ALOC or SHOCK

Shock...not that shock
- Just to emphasize!
- ALOC, signs and symptoms of shock such as tachycardia, hypotension, diaphoresis, decreased pulses, and pallor have PRIORITY.
- I hope you think this is obvious by now.
- A new postoperative client has priority over clients who have been in the hospital for a few days, unless, of course, their condition has changed and have become unstable.
- Also, clients that require temporary monitoring such as a client who had sedation/anesthesia during a procedure have PRIORITY.
NEW ADMISSIONS
- New admissions have priority over clients who are ready to be discharged.
ALARMING or MALFUNCTIONING equipment

- Equipment such as ventilators, pacemakers, or IV pumps with critical meds are priority. If a cardiac monitor is alarming, go see that client first. He or she may be in cardiac arrest or other deadly heart rhythm. If an IV alarm is beeping and the patient is getting a caustic medication (a medication that burns skin) if it infiltrates, go see that patient.

The Simple Terms
- Airway
- Breathing
- Circulation
- Unexpected Symptoms
- Chest Pain
- Deadly Labs
- Unstable
- Bleeding
- Acute over chronic
- ALOC
- Shock
- New post-op
- New Admissions
- Malfunctioning or alarming equipment
What you have been waiting for! Let's test your prioritizing skills.
- The goal of this module is to teach you how to prioritize; however, every question is a learning experience that addresses knowledge that is frequently tested in the NCLEX. Be ready to get the other modules as they become available to get your fully prepared for the NCLEX-RN!
Quiz Summary
0 of 35 Questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 35 Questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- 33
- 34
- 35
- Current
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 35
1. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 2 of 35
2. Question
The nurse is working in the emergency department. She has 4 clients she needs to assess. Which client should the nurse assess FIRST?
CorrectIncorrect -
Question 3 of 35
3. Question
Let’s go simple. Is this client having EXPECTED or UNEXPECTED/COMPLICATION symptoms?
A client with a history hyperthyroidism who had right hip replacement is complaining of feeling hot, has tachycardia and palpitations, and is very confused.
CorrectIncorrect -
Question 4 of 35
4. Question
A client who just had a right chest tube due to a pneumothorax has tidaling and small amount of intermittent bubbling in the water seal chamber.
CorrectIncorrect -
Question 5 of 35
5. Question
The nurse is working in the emergency department. Which client should the nurse assess FIRST?
CorrectIncorrect -
Question 6 of 35
6. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 7 of 35
7. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 8 of 35
8. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 9 of 35
9. Question
Who should the ER nurse assess FIRST?
CorrectIncorrect -
Question 10 of 35
10. Question
Who should the nurse see FIRST?
CorrectIncorrect -
Question 11 of 35
11. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 12 of 35
12. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 13 of 35
13. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 14 of 35
14. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 15 of 35
15. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 16 of 35
16. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 17 of 35
17. Question
Which of the following clients should the nurse assess first?
CorrectIncorrect -
Question 18 of 35
18. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 19 of 35
19. Question
Which client should the nurse assess FIRST?
CorrectIncorrect -
Question 20 of 35
20. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 21 of 35
21. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 22 of 35
22. Question
Which of the following clients needs follow up?
CorrectIncorrect -
Question 23 of 35
23. Question
Which of the following clients should the nurse help first?
CorrectIncorrect -
Question 24 of 35
24. Question
Which of the following clients should the trauma nurse assess First?
CorrectIncorrect -
Question 25 of 35
25. Question
Which of the following clients needs follow up by the hemodialysis nurse?
CorrectIncorrect -
Question 26 of 35
26. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 27 of 35
27. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 28 of 35
28. Question
The nurse has been made aware of the following client situations. Which client needs immediate follow up?
CorrectIncorrect -
Question 29 of 35
29. Question
Which of the following clients requires immediate follow up?
CorrectIncorrect -
Question 30 of 35
30. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 31 of 35
31. Question
Which of the following clients should the nurse see FIRST?
CorrectIncorrect -
Question 32 of 35
32. Question
Which of the following clients should the nurse assess FIRST?
CorrectIncorrect -
Question 33 of 35
33. Question
Which of the following clients should the nurse assess First?
CorrectIncorrect -
Question 34 of 35
34. Question
Which of the following clients should the RN assess first?
CorrectIncorrect -
Question 35 of 35
35. Question
Which of the following clients should the nurse assess first?
CorrectIncorrect